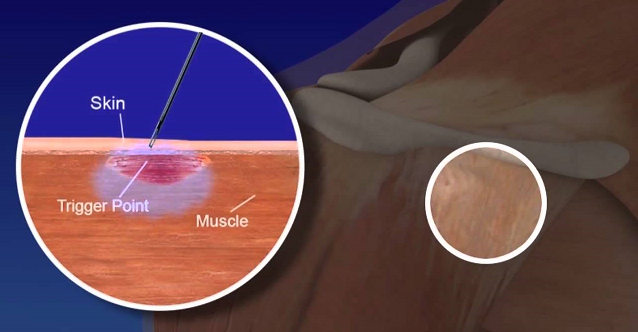
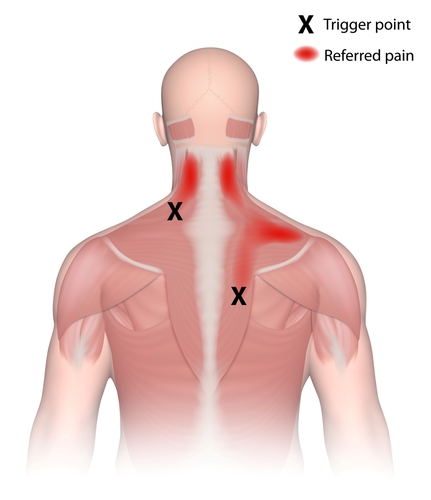
Myofascial trigger points
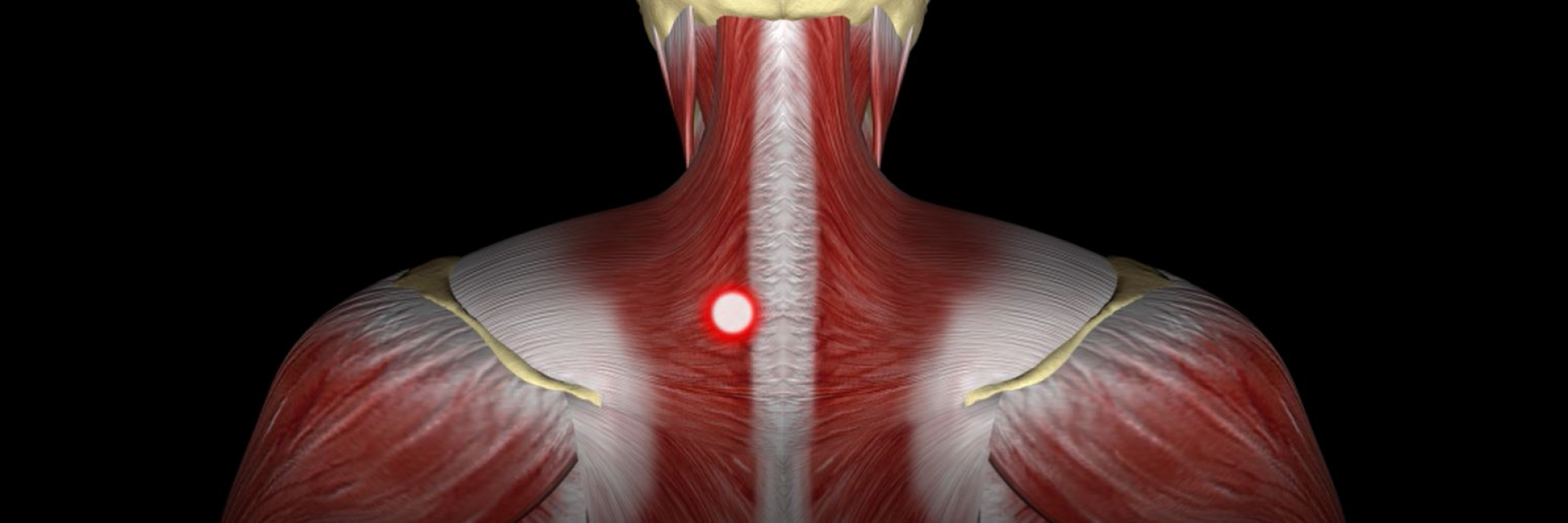
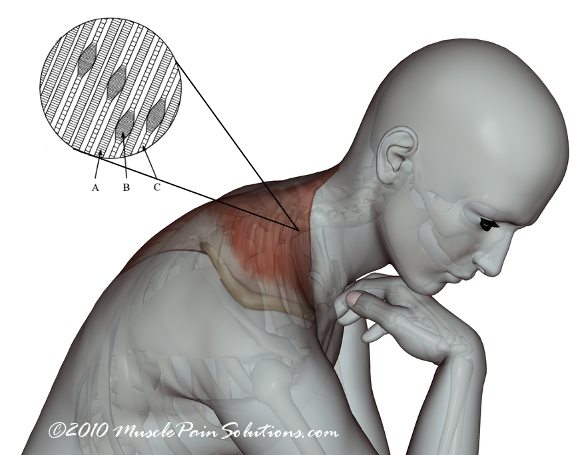
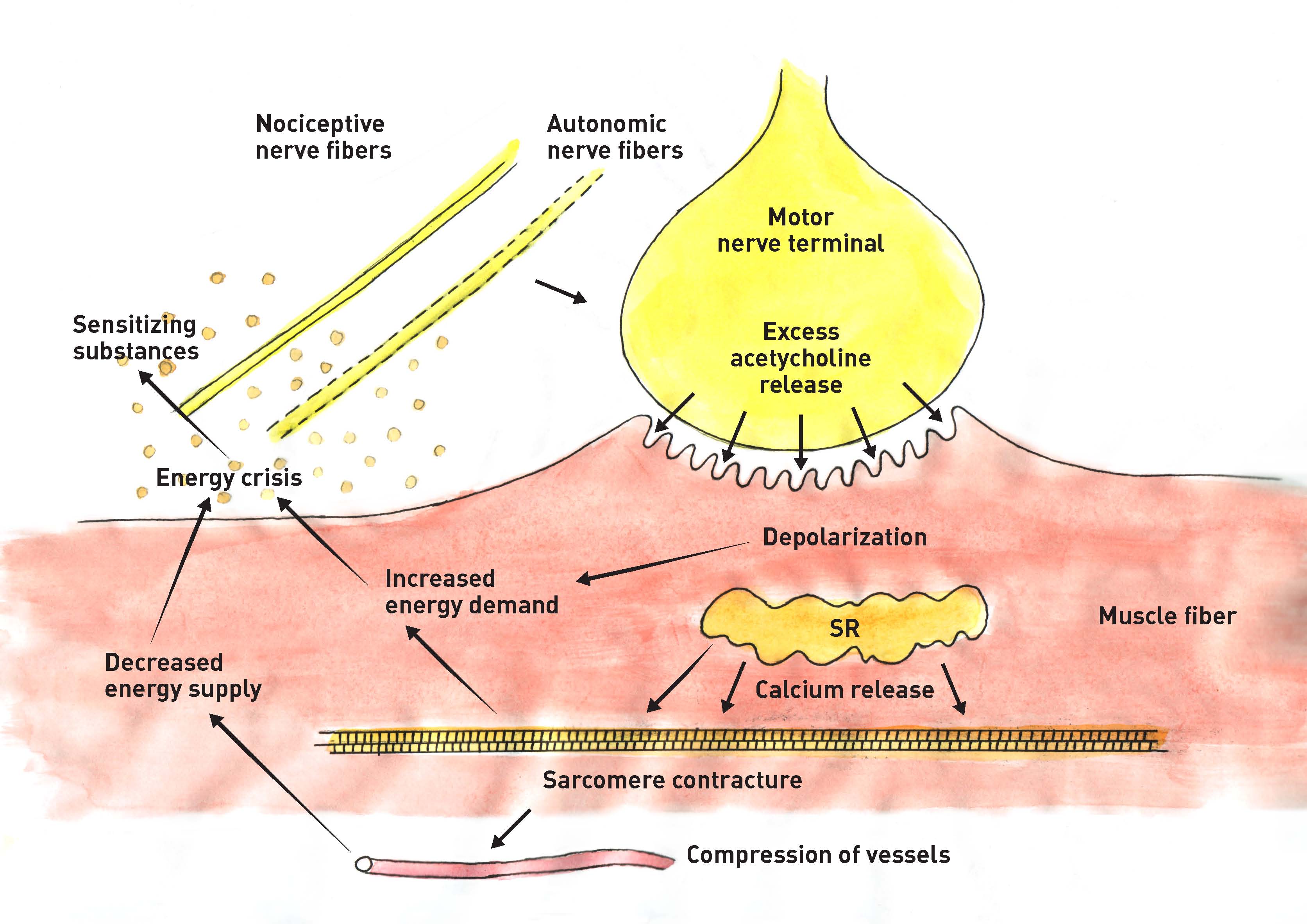
Diagnosis is clinical and includes the identification of small knots (2-5 mm in diameter) and tight bands within affected muscles that are painful when palpated. Diagnostic imaging is not helpful and should only be considered to rule out other causes of muscle pain. It is still unclear whether or not myofascial trigger points are true pathologic entities. It has been hypothesized that muscle injury or stress disrupts the sarcoplasmic reticulum within muscle fibers, releasing free calcium ions. These free calcium ions causes the actin and myosin of the muscle fibers to lock into place as long as adenosine triphosphate is available. The resulting contraction of small parts of the muscle leads to diminished blood flow with subsequent ischemia and release of painful substances such as serotonin, histamine and prostaglandins in the affected area. Myofascial trigger points are a very common condition, especially in the cervical musculature. Up to 85% of back pain and approximately 55% of neck pain and headaches are caused by myofascial pain. The predominant age of patients suffering from myofascial trigger pointsis 30 to 50 years. Women are more affected than men. Very often Myofascial trigger points are associated with poor posture. Notably, myofascial trigger pointss frequently produce neurological complaints including headache, dizziness, sensory symptoms, as well as gastrointestinal problems. The treatment of Myofascial trigger points should start with a manual technique that involves applying pressure to a trigger point to release the pathologic contraction of the muscle segment and to stretch the segment to restore normal muscle fiber length. This can be accompanied by acupuncture, stress management and relaxation techniques. Pharmacologic treatment is unspecific and may comprise muscle relaxants, nonsteroidal anti-inflammatory drugs (NSAIDs), anticonvulsants, or topical application of local anesthetics or botulinum toxin. Radial shock wave therapy is very effective for Myofascial trigger points and may mimic manual therapy in applying pressure to a trigger point to release the pathologic contraction of the muscle segment. Prevention of recurrence should focus on appropriate ergonomic changes in patients’ day-to-day activities to avoid repetitive stress to the injured muscles. Side effects of Radial Shock Wave Therapy (RSWT) using the Swiss DolorClast®. When performed properly, RSWT with the Swiss DolorClast® has only minimal risks. Typical device-related non-serious adverse events are: Pain and discomfort during and after treatment (anesthesia is not necessary) Reddening of the skin Petechia Swelling and numbness of the skin over the treatment area These device-related non-serious adverse events usually disappear within 36h after the treatment.
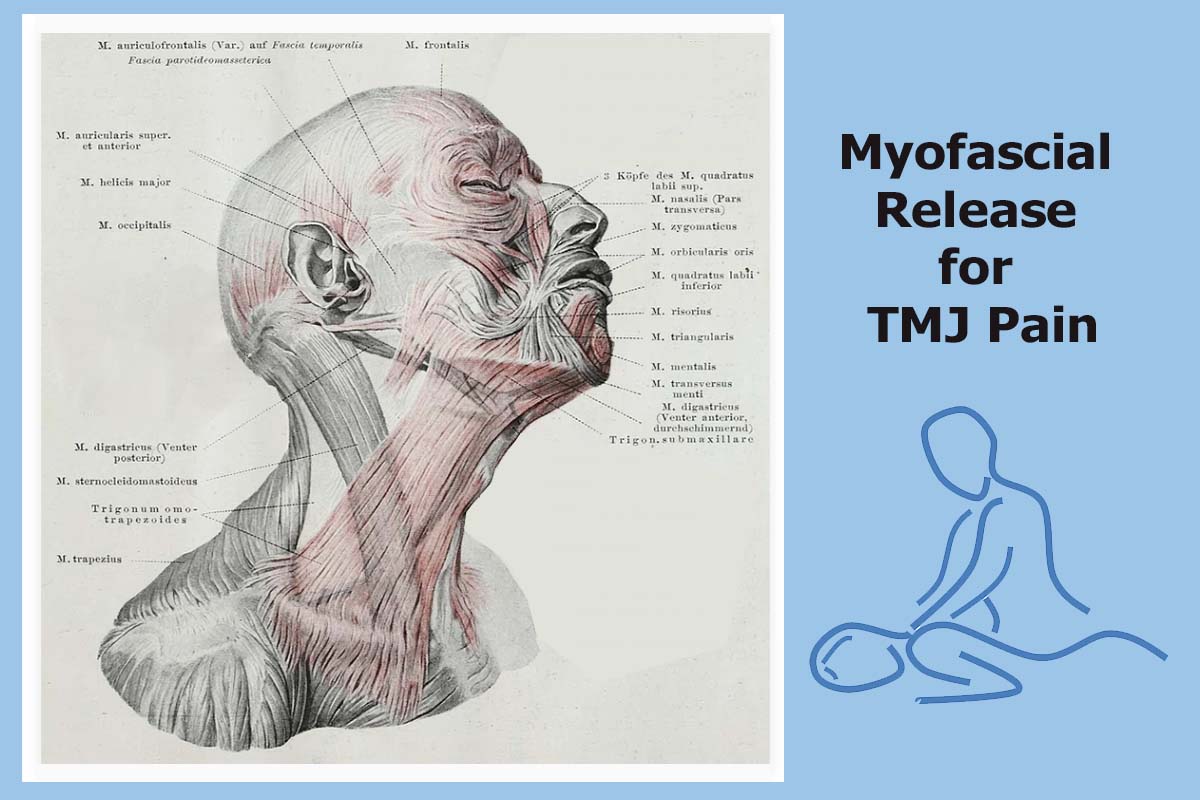
Myofascial Release Treatment for TMJ Pain
Hilterapia® is effective for treating myofascial trigger points

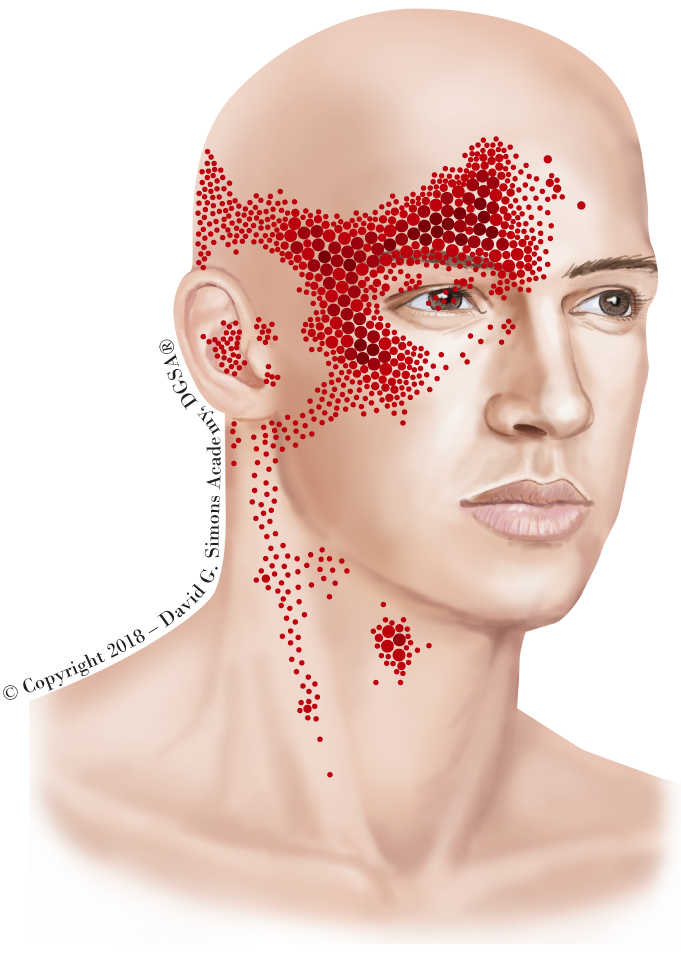
PDF] Myofascial Trigger Points and Sensitization: An Updated Pain Model for Tension-Type Headache
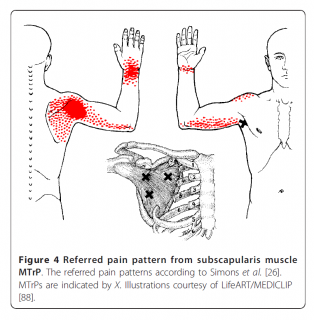
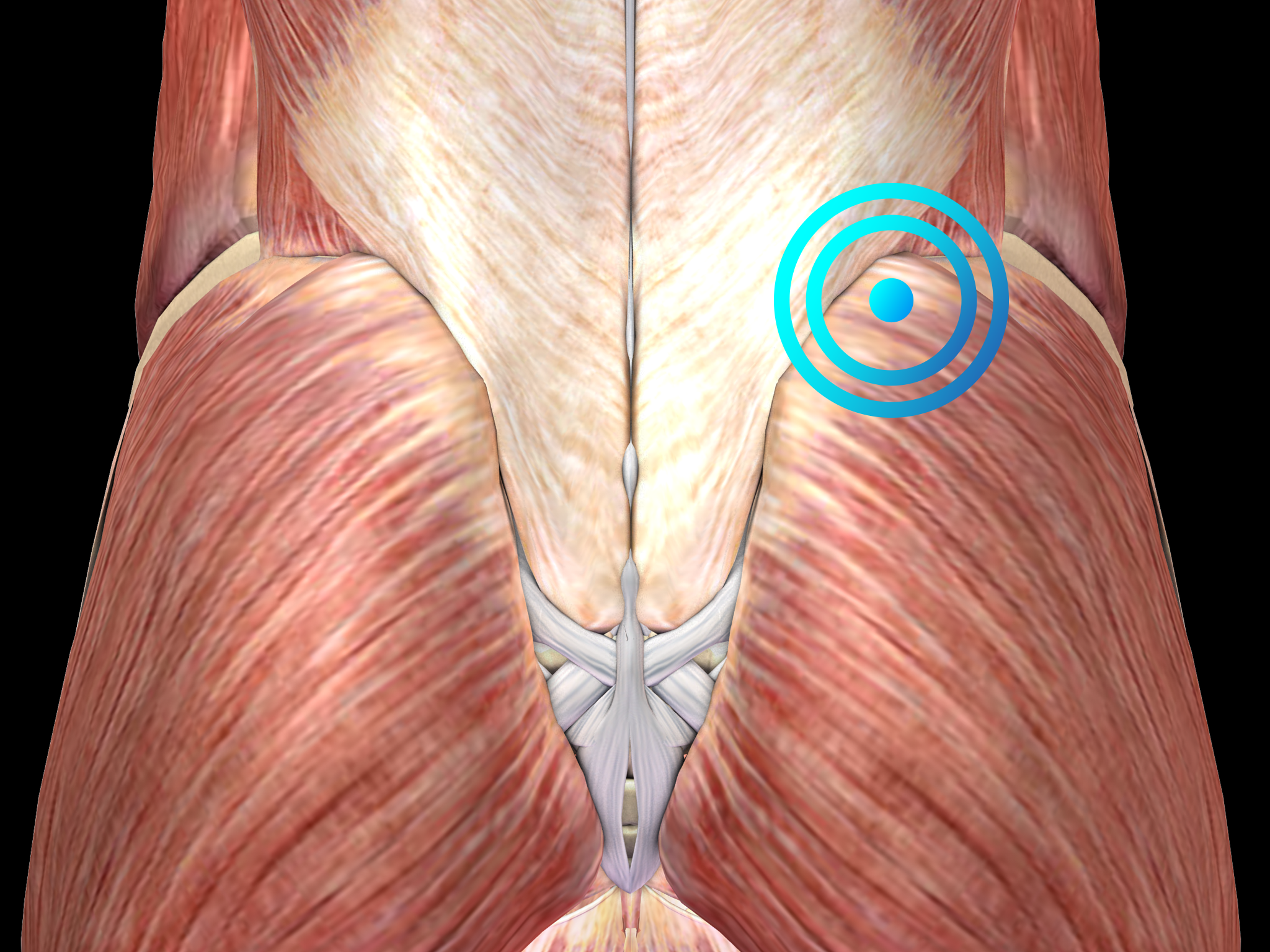
Can (myofascial) trigger points cause shoulder pain Can (myofascial) trigger points cause shoulder pain
Myofascial trigger points
Myofascial Trigger Points
Myofascial Trigger Points: we have been studying them since 1995: David G. Simons Academy, DGSA®
Myofascial Trigger Points: we have been studying them since 1995: David G. Simons Academy, DGSA®

Myofascial Release Trigger Point Release New York, Roadside Physical Therapy

Myofascial Trigger Points Chart Trigger points, Myofascial pain, Myofascial
Trigger Points – Adam Fields

Myofascial Pain Syndrome and Trigger Points Treatments, Animation.

Myofascial Pain Syndrome Trigger Points Chart